
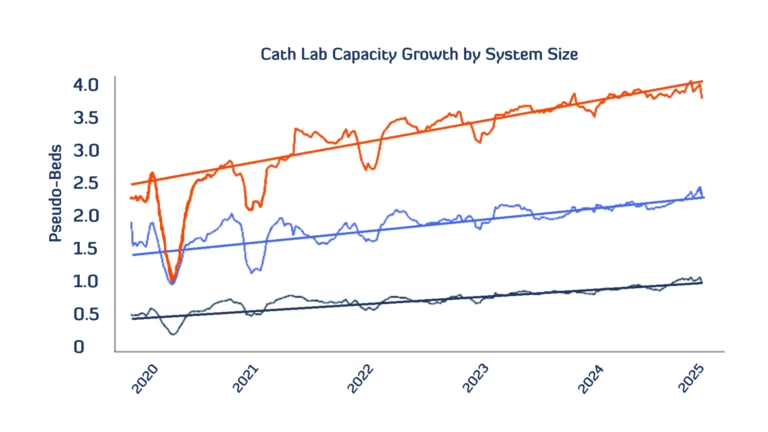
Cath Lab Capacity is Up—But Structural Heart Procedures Are Being Outpaced by Other Interventions
Heart failure with a preserved ejection fraction (HFpEF) accounts for more than half of all heart failure cases and carries significant morbidity and mortality risk, especially after hospitalization1. Historically, management of the disease is largely focused on comorbidity management and lifestyle modifications, given that available therapies had not demonstrated sufficient

From Black Box to Breakthrough: Unlocking Hidden Care Patterns with LLM-Enriched Data
Heart failure with a preserved ejection fraction (HFpEF) accounts for more than half of all heart failure cases and carries significant morbidity and mortality risk, especially after hospitalization1. Historically, management of the disease is largely focused on comorbidity management and lifestyle modifications, given that available therapies had not demonstrated sufficient

SGLT2i + GLP-1 RA: A Dynamic Duo in HFpEF?
Heart failure with a preserved ejection fraction (HFpEF) accounts for more than half of all heart failure cases and carries significant morbidity and mortality risk, especially after hospitalization1. Historically, management of the disease is largely focused on comorbidity management and lifestyle modifications, given that available therapies had not demonstrated sufficient
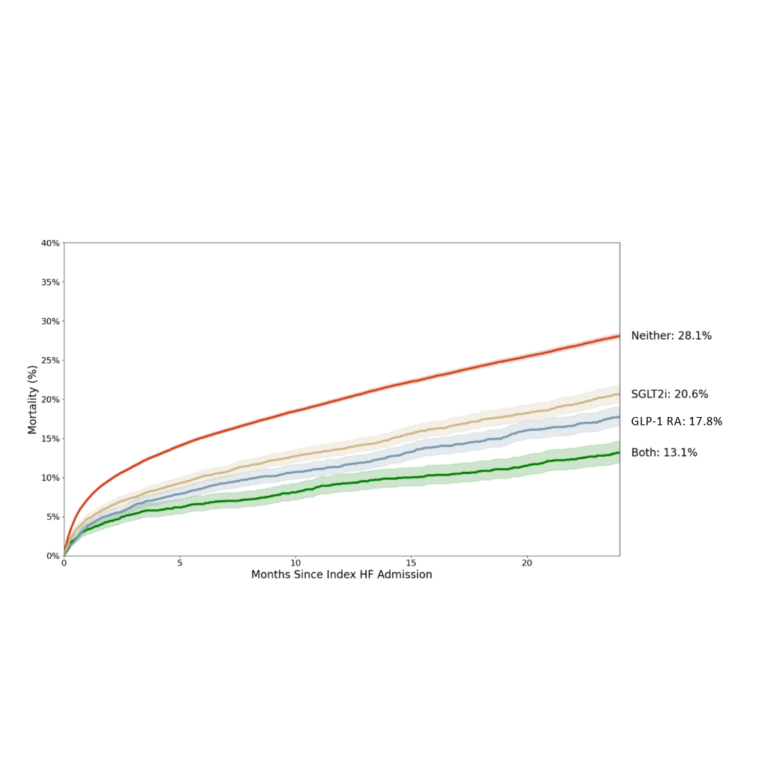
Two-Year Mortality Following Heart Failure Hospitalization in Patients with HFpEF Stratified by SGLT2i and GLP-1 RA Therapy: A Real-World Analysis
BACKGROUND Heart failure with a preserved ejection fraction (HFpEF) is characterized by frequent hospitalizations, and substantial mortality. While historically lacking effective therapies, newer treatments, including SGLT2 inhibitors (SGLT2i) and GLP-1 receptor agonists (GLP-1 RA), have shown potential benefits. However, the clinical course of HFpEF under these therapies remains incompletely characterized,

What the EARLY TAVR Trial Data Could Mean for Already Busy Heart Teams
On the heels of the exciting EARLY TAVR data and egnite’s Acute Valve Syndrome in Aortic Stenosis study, both led by Dr. Philippe Genereux, we’ve been asked by several cardiovascular (CV) administrators what a potential change in the management of asymptomatic severe aortic stenosis (SAS) patients could mean for their