egnite Research
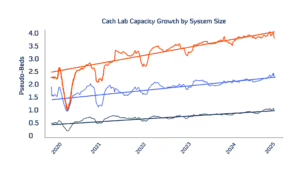
Cath Lab Capacity is Up—But Structural Heart Procedures Are Being Outpaced by Other Interventions
Heart failure with a preserved ejection fraction (HFpEF) accounts for more than half of all heart failure cases and carries significant morbidity and mortality risk, especially after hospitalization1. Historically, management of the disease is largely focused on comorbidity management and lifestyle modifications, given that available therapies had not demonstrated sufficient impact on hospitalization burden or mortality. In recent years, however, the treatment paradigm for HFpEF has shifted, with a growing emphasis on SGLT2 inhibitors (SGLT2i). Originally developed to lower blood glucose levels in diabetic patients, several clinical trials have firmly established that SGLT2i is also beneficial for patients living with HFpEF2.